
Addiction Treatment Program
Our addiction treatment negates patients' need to abuse drugs and alcohol to feel normal.
America’s addiction treatment centers misdiagnose 80% of their addicted patients – they fail to diagnose the underlying medical and biochemical disorders that change brain chemistry, causing drug cravings.
When Sponaugle Wellness patients relapse, it is most often because they don’t return for follow-up visits that allow us the ability to finish the job.
Others fail to take advantage of our anti-aging, brain, and body wellness program, including addiction treatment. This program not only stops drug and alcohol cravings, but it also accelerates the healing of our patient’s brains and bodies. Our middle-aged patients typically look and feel ten years younger within just four weeks*.

What is Addiction?
Our patients are successful in achieving 9% relapse rates as compared to 80% national relapse rates due to our approach to treatment.
The White House invited Dr. Rick Sponaugle to speak on scientific addiction treatment. At Sponaugle Wellness Institute, the team integrates modern brain science with wellness medicine to balance and optimize brain function; this stops craving for drugs and alcohol.
Dr. Sponaugle was invited to the White House to explain how and why his science-based addiction treatment achieves 90 percent success rates compared to 10 percent success rates at America’s traditional rehab centers.
Dr. Sponaugle explained to Deputy Chief Rubin Brazalis and the White House staff that the knowledge gained from his addiction research and that from scientists at the National Institute of Drug Addiction enabled him to stop the “biochemical” drug craving in his addicted patients.
Dr. Sponaugle further explained that AA-based, 12-step programs attempt to coach patients through each day of craving, leaving patients a set up for failure because they have to “white knuckle” through each day of craving.
Dr. Sponaugle explained that drug craving is biochemical and that patients will crave the biochemical effect of any drug that temporarily balances their brain chemistry.
He further explained that when the underlying cause[s] of biochemical craving is diagnosed and subsequently treated, addicted patients no longer need or crave drugs.
Dr. Sponaugle enlightened the White House staff regarding the many medical disorders he discovered can cause drug cravings. These disorders range from inherited brain chemical deficiencies to pituitary tumors. These medical disorders are routinely overlooked at America’s rehab centers because they are too focused on talk therapy.
Dr. Sponaugle emphasized that there is no “disease of addiction,” a common myth propagated by addiction doctors. Rather, many disease states cause drug cravings and lead to addiction.
Patients are misdiagnosed as “drug addicts” by addiction specialists who lack adequate brain physiology and biochemistry knowledge. Dr. Sponaugle explained to Bush’s deputy chief that he diagnoses medical disorders in patients who have attended 12 or more rehab centers only to be misdiagnosed as a drug addicts.
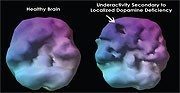
America’s addiction doctors misunderstand that patients use drugs and alcohol to balance their brain chemistry, not to get high. Dr. Sponaugle explained that some patients are trying to get high-er, to a normal if they have inherited an underactive reward center. This phenomenon is called Reward Deficiency Syndrome.
Other patients use drugs to quiet their overactive brain regions. Unfortunately, over time, the drugs used by patients to self-medicate will actually distort their brain chemistry to a greater extent than what they inherited. Their drug induced hormonal and nutritional deficiencies worsen drug and alcohol craving.
America’s addiction treatment centers fail to diagnose and treat drug induced deficiencies of brain chemicals, hormones and amino acids, therefore, patients fall into a “black hole” immediately following their drug detox. The black hole is described by alcoholics as the “dry drunk” syndrome. The “black hole” is the reason that sixty percent of America’s addicted patients relapse within four weeks of their detox!
At Sponaugle Wellness Institute, Dr. Sponaugle begins correcting brain chemistry, hormonal and nutritional [amino acid] deficiencies during the patient’s drug detoxification process. He corrects over 65 biochemical deficiencies in the average addicted patient, many come in on Monday feeling depressed and suffering fatigue, but, they leave the detox unit on Friday feeling and looking 10 years younger.
Dr. Sponaugle Explains The Brain Chemistry of Addiction
Our patients are successful in achieving 9% relapse rates as compared to 80% national relapse rates due to our approach to treatment.
The White House invited Dr. Rick Sponaugle to speak on scientific addiction treatment. At Sponaugle Wellness Institute, the team integrates modern brain science with wellness medicine to balance and optimize brain function; this stops craving for drugs and alcohol.
Dr. Sponaugle was invited to the White House to explain how and why his science based addiction treatment achieves 90 percent success rates* as compared to 10 percent success rates at America’s traditional rehab centers.
Dr. Sponaugle explained to Deputy Chief Rubin Brazalis and the White House staff that the knowledge gained from his addiction research and that from scientists at the National Institute of Drug Addiction enabled him to stop the “biochemical” drug craving in his addicted patients.
Dr. Sponaugle further explained that AA based, 12-step programs attempt to coach patients through each day of craving leaving patients a set up for failing because they have to “white knuckle” through each day of craving.
Dr. Sponaugle explained that drug craving is actually biochemical in nature and that patients will crave the biochemical effect of any drug that temporarily balances their brain chemistry. He further explained that when the underlying cause[s] of biochemical craving is diagnosed and subsequently treated, addicted patients no longer need or crave drugs.
Dr. Sponaugle enlightened the White House staff regarding the many different medical disorders he has discovered can cause drug craving. These disorders range from inherited brain chemical deficiencies to pituitary tumors. This medical disorders are routinely overlooked at America’s rehab centers because they are too focused on talk therapy.
Dr. Sponaugle emphasized that there is no “disease of addiction,” a common myth propagated by addiction doctors. Rather, there are many disease states that cause drug craving and lead to addiction.
Patients are misdiagnosed as “drug addicts” by addiction specialists who lack adequate knowledge of brain physiology and biochemistry. Dr. Sponaugle explained to Bush’s deputy chief that he diagnoses medical disorders in patients who have attended 12 or more rehab centers only to be misdiagnosed as a drug addict.
America’s addiction doctors misunderstand the concept that patients use drugs and alcohol to balance their brain chemistry, not to get high. Dr. Sponaugle explained that some patients are trying to get high-er, to a normal if they have inherited an underactive reward center. This phenomenon is called Reward Deficiency Syndrome.
Other patients use drugs to quiet their overactive brain regions. Unfortunately, over time, the drugs used by patients to self-medicate will actually distort their brain chemistry to a greater extent than what they inherited. Their drug induced hormonal and nutritional deficiencies worsen drug and alcohol craving.
America’s addiction treatment centers fail to diagnose and treat drug induced deficiencies of brain chemicals, hormones and amino acids, therefore, patients fall into a “black hole” immediately following their drug detox. The black hole is described by alcoholics as the “dry drunk” syndrome. The “black hole” is the reason that sixty percent of America’s addicted patients relapse within four weeks of their detox!
At Sponaugle Wellness Institute, Dr. Sponaugle begins correcting brain chemistry, hormonal and nutritional [amino acid] deficiencies during the patient’s drug detoxification process. He corrects over 65 biochemical deficiencies in the average addicted patient, many come in on Monday feeling depressed and suffering fatigue, but, they leave the detox unit on Friday feeling and looking 10 years younger.



Optimizing Dopamine Activity
When our wellness center treats neurotoxicity and optimizes dopamine activity in the dopamine-driven hunger/reward center these patients no longer suffer excessive craving for food. They can then metabolize fat at a much faster rate as they did in high school. More importantly, our comprehensive anti-aging program reverses brain and body aging by 10 to 15 years, depending on the age of the patient*.
Our facility uses the same protocol to treat Alzheimer’s, Autism, and Multiple Sclerosis. We recently used our Alzheimer’s protocol to awaken a 94-year-old Clearwater man from his two year cognitive coma*. Reducing our patients’ risk of developing Alzheimer’s disease is so important because Alzheimer’s disease has doubled since 1980. Brain scientists suggest that by 2025 one-half of Americans in their mid-fifties will suffer Alzheimer’s symptoms if Americans don’t make some necessary changes.

Getting Healthy Naturally
By the end of the anti-aging/wellness program, our female patients effortlessly lose the extra 30 pounds they gained since high school*. Our post addiction outpatient drug rehab optimizes our patient’s brain function correcting multiple drug and alcohol-induced hormonal and vitamin deficiencies, and it provides detoxification of neurotoxins that accumulate in the brain of all Americans.
These fatty toxins shut down the brain’s hunger center causing food cravings. Many 300 pound female patients who suffered life long weight problems lose 70 pounds within three months from their detox and wellness treatment date*. Dr. Sponaugle diagnoses many of these women with an underactive nucleus accumbens, the brain region that serves as our hunger and reward center.
These patients eat to stimulate their underactive nucleus accumbens, eating temporarily [90 minutes] makes them feel less depressed. Patients who suffer obesity because of an underactive nucleus accumbens are rarely diagnosed by eating disorder “specialists” because they don’t realize these patients eat to get closer to normal. These patients also suffer seasonal affective disorder (SAD) and they tend to eat more in the winter when skies turn gray in northern latitudes.
American women develop more gastrointestinal dysbiosis than men and therefore suffer more accumulation of gut-derived fatty toxins in their brains. These toxins accumulate slowly and over time suppress hormonal output and disrupt brain chemistry circuits. This causes the brain’s hunger center to down-regulate in activity producing food cravings, especially for foods that contain high levels of tyrosine, like chocolate.
Drug Addiction Treatment

Despite a trillion dollars having been spent on this nation’s “drug wars” over the past six decades, more addictive and lethal compounds are used by Americans than ever before.
Why are we losing the war against drug addiction? One pioneering physician has a simple answer.
Life Extension® recently had the opportunity to speak at length with Dr. Sponaugle. Dr. Sponaugle rejects addiction treatment that is based solely on counseling, the preferred methodology among almost all drug treatment facilities in the United States (97%).4
Instead, he combines state-of-the-art technology with safe, low-cost, natural interventions, including hormones, supplements, and restoration of gut ecology. The efficacy of his approach speaks for itself. While national relapse rates range as high as 90% by some estimates,5,6 Dr. Sponaugle has treated over 5,000 substance abusers—with a relapse rate of only 9%!
Novel Methods to Cure Drug Addiction
By Mark Joslin
There is a drug-induced death in this country every 15 minutes1, a trend that has risen steadily over the past decade. Despite a trillion dollars2 having been spent on this nation’s “drug wars” over the past six decades, more addictive and lethal compounds are used by Americans than ever before.3
Why are we losing the war against drug addiction? One pioneering physician has a simple answer.
Life Extension® recently had the opportunity to speak at length with Dr. Marvin “Rick”
Sponaugle. Sponaugle rejects addiction treatment that is based solely on counseling, the preferred methodology among almost all drug treatment facilities in the United States (97%).4
Instead, he combines state-of-the-art technology with safe, low-cost, natural interventions, including hormones, supplements, and restoration of gut ecology. The efficacy of his approach speaks for itself. While national relapse rates range as high as 90% by some estimates,5,6 Dr. Sponaugle has treated over 5,000 substance abusers—with a relapse rate of only 9%!7*
According to Dr. Sponaugle, most detox and rehab programs are ineffective because they do not address the root problem. “Patients continue to relapse until their brain function is optimized. Otherwise, patients will continue to use drugs to stimulate underactive brain regions and to calm overactive brain regions. We have learned that successful addiction treatment requires diagnosis and treatment of multiple underlying biochemical and medical disorders.”
Official statistics support Sponaugle’s contention. The National Institutes of Health report that long-term drug abuse induces adverse chemical alterations in the brain that remain long after someone has stopped using drugs.6 This simple fact supports a multi-targeted neurochemical intervention over behavioral approaches like counseling.
Addiction Statistics: USA |
||||||||||||||||||||
|
Inherited Abnormalities in Brain Chemistry
According to Sponaugle, the overwhelming majority of his 5,000 successfully treated patients have areas of their brains that are either overactive or underactive.7 And that abnormal activity level helps determine the kind of drug, substance, or behavior a person may turn to in order to “normalize” their feelings.
The underactive areas most commonly involve the prefrontal cortex (brain region behind the forehead) and the pleasure or reward system of the brain. People with diminished activity in the nucleus accumbens (reward center) display what scientists call “reward deficiency syndrome,” or RDS.16 People with RDS have a hard time feeling “normal” responses to positive events, leaving them essentially hungering for happiness. Neurons in those low-activity areas are primarily driven by the neurotransmitter dopamine; addicts tend to display marked deficiencies in dopamine activity in both areas.17-19
As a result, says Dr. Sponaugle, people with RDS often seek to rebalance their brains with stimulating substances or behaviors that produce a dopamine surge in their pleasure center.7 For example, these patients might become addicted to cocaine, opiate drugs such as morphine or heroin, or stimulants such as amphetamines.
Dr. Sponaugle has demonstrated these effects graphically in a series of SPECT scans on his patients with addictions to cocaine and OxyContin®: all of them showed a marked reduction in the activity of neurons that rely on dopamine. Dr. Sponaugle refers to these areas as “dopamine holes,” and he uses them as a diagnostic feature as he seeks to rebalance his patients’ brain chemistry.
People with overactive brain regions have an entirely different set of problems and are likely to become addicted to “calming” substances, according to Dr. Sponaugle.7 Neurotransmitters involved in these areas are excitatory chemicals such as dopamine, histamine, glutamate, epinephrine (adrenalin) and norepinephrine.20 Their effect is to increase the electrical activity of brain cells. At low levels of excess activity, patients may experience mild anxiety or insomnia. At higher levels, they may experience panic attacks or even live in a more or less continuous panic mode.7
This increased activity also shows up on SPECT scans, most notably in patients with high levels of anxiety or with panic disorders.21-23 Histamine is especially active in such patients’ brains. 24-26 Dr. Sponaugle has a large file of SPECT scans showing overactive brain regions derived from elevated histamine activity in his patients addicted to “calming” substances such as alcohol, benzodiazepine anti-anxiety medications (e.g., Valium® or Xanax®), and again, opiates.
Dr. Sponaugle’s Approach to Curing Addiction
- Conventional addiction treatment using psychotherapy, medications, shock therapy, and painful detox programs often yields disappointing results.
- Up to 90% of those who attempt to overcome an addiction relapse*.
- This may be because long-term drug use creates long-lasting changes in brain chemistry.
- Dr. Marvin “Rick” Sponaugle has developed an effective, integrative addiction recovery program that addresses the brain imbalances at the root of addictions.
- Addressing inherited and acquired brain chemistry patterns is crucial to achieving lasting addiction recovery.
- Inherited addiction tendencies can involve areas of the brain that are overactive or underactive.
- Acquired hormone and gut imbalances can disrupt brain chemistry, setting the stage for addiction.
- Dr. Sponaugle restores optimal nutrient levels, hormones, enzymes, brain chemicals, and gastrointestinal health to help people overcome addiction— with a remarkable relapse rate of only 9%.*
Acquired Abnormalities in Brain Chemistry
According to Dr. Sponaugle, people are “set up” for addictions by their inherited brain chemistry patterns. But that alone is not always enough to trigger an addiction. A “second hit” is usually required, typically in the form of imbalances in two important biological areas, the intestine and the endocrine (hormonal) system.
Gut Imbalance
 The human gut is frequently referred to as the “second brain” because of its normally high production of serotonin and other neurotransmitters.27
The human gut is frequently referred to as the “second brain” because of its normally high production of serotonin and other neurotransmitters.27
Sponaugle says his clinical research suggests that “Toxins from the gut more frequently cause addiction than from any other single causation.”7
Alterations in the patterns of intestinal bacteria, coupled with ingestion of toxins from the environment, can produce what is known as intestinal hyperpermeability or “leaky gut,” a damaged intestinal lining that allows substances that normally would be eliminated in the stool to be absorbed into the bloodstream, with consequences in the brain.28,29
Bacterial overgrowth in the gut may also interfere with serotonin.30 According to Dr. Sponaugle, food allergies cause elevated histamine levels that lead to increased electrical activity throughout the brain. Histamine’s chemical structure is closely related to dopamine, and Dr. Sponaugle believes that histamine stimulates dopamine activity in the brain.
Dr. Sponaugle says that in his clinical experience, “alcoholism is linked with overgrowth of candida in the gastrointestinal tract.” He has observed that this GI disturbance is linked with deficiencies of two calming brain chemicals: serotonin and taurine. The combination of serotonin deficiency, taurine deficiency, and excessive histamine activation keeps the alcoholic in a state that feels like a constant alcohol-withdrawal pattern, says Dr. Sponaugle. “The need to drink becomes more intense, causing increased anxiety and insomnia.”
Hormonal Imbalance
Dr. Sponaugle says that his clinic has found hormonal imbalances to be one of the most common causes of addiction in middle-aged women. This is hardly surprising, since hormones such as estrogen, progesterone, and pregnenolone are known to have powerful effects on brain function, yet traditional centers fail to evaluate female hormones. These “neurosteroids” are potent modulators of the neurotransmitters dopamine, serotonin, and gamma-aminobutyric acid (GABA), so when a woman’s hormones are out of balance, so is the electrical activity in her brain. 31-33
Estradiol, for example, increases serotonin receptor activity in the brain.34 That contributes to a sense of well-being that can be rapidly lost in the premenstrual period and at the onset of menopause when estrogen levels plummet. These are also the times in a woman’s life when she is most likely to suffer from depression, anxiety, and insomnia—all of which can be “self-medicated” with chemical substances that transiently “quiet” overactive brain regions: alcohol, Xanax®, and even opiate pain medication.
Dr. Sponaugle’s Approach to Diagnosis and Treatment
 Dr. Sponaugle’s unique approach focuses on determining abnormal brain chemistry patterns and then rectifying them. In order to correctly assess biochemical and medical disorders that can distort brain chemistry and cause various addiction and anxiety issues, Sponaugle conducts a comprehensive analysis of more than 65 brain chemicals, hormones, enzymes, toxins, amino acids, infectious biomarkers, and vitamins through blood and urine testing.
Dr. Sponaugle’s unique approach focuses on determining abnormal brain chemistry patterns and then rectifying them. In order to correctly assess biochemical and medical disorders that can distort brain chemistry and cause various addiction and anxiety issues, Sponaugle conducts a comprehensive analysis of more than 65 brain chemicals, hormones, enzymes, toxins, amino acids, infectious biomarkers, and vitamins through blood and urine testing.
This extensive evaluation allows Sponaugle to determine the root causes of each individual’s addictive behaviors. The possibilities of exposure to mold and industrial toxins are also evaluated in many cases.
Dr. Sponaugle is critical of conventional addiction treatment programs, noting that most focus only on one or two aspects of drug addiction.
Instead, Sponaugle uses a combination of treatments he refers to as nutritional and rapid detox. Sponaugle’s nutritional detox provides intravenous amino acids, vitamins, and minerals to remedy biochemical imbalances safely.
Dr. Sponaugle drew on his extensive anesthesia and intensive care training to develop his rapid detox protocol. In this phase, he administers intravenous (IV) sedation and other medications that help blunt or block physical withdrawal symptoms. These symptoms are typically related to elevated levels of “fight or flight” hormones like adrenaline that produce anxiety, agitation, palpitations, and jitteriness. Those unpleasant feelings, left uncorrected, make the detox experience so uncomfortable that many addicts prefer the addiction.
Dr. Sponaugle customizes his protocol to each patient, which helps him avoid any of the effects of the withdrawal-related adrenaline surge. His continued assessment and balancing of hormone and neurotransmitter levels over the longer term enables his patients’ recovery process to be more effective.
A Look at Dr. Sponaugle’s Casebook
Two cases from Dr. Sponaugle’s clinical experience serve to illustrate his approach.
Jennifer*
Jennifer was a 54-year-old nurse who began drinking large amounts of wine at age 50 (she had previously been a light social drinker only). On arrival at Dr. Sponaugle’s clinic, she had just returned from a 28-day, $46,000 stay at a treatment center in Arizona, relapsing just four days after returning home.
Jennifer’s brain scan revealed both areas of low dopamine activity (dopamine holes in her prefrontal cortex) and an overactive deep limbic region linked with serotonin and taurine deficiency. Her brain scan revealed generalized overactivity, likely due to elevated histamine from her leaky gut syndrome. Her urinary neurotransmitter testing revealed low serotonin and taurine levels, and a markedly elevated histamine level, vividly demonstrating brain chemical imbalances associated with excessive wine consumption.
Complicating her alcohol-related serotonin deficiency was Jennifer’s menopausal low estradiol levels, making her brain resistant to what serotonin she did produce. The Arizona treatment center had started her on serotonin-boosting SSRI (selective serotonin reuptake inhibitor) medication [Lexapro®], but it had no effect on her menopausal serotonin-resistant receptors.
The net result, says Dr. Sponaugle, was an overactive limbic system creating a steady beat of depression and anxiety. It is hardly surprising that without further treatment, Jennifer quickly resorted to self-medication with her drug of choice: alcohol.
Jennifer was started on high-quality supplements including 5-hydroxytryptophan (5-HTP), allowing her brain to begin making more serotonin. She was also given appropriate estradiol replacement to restore her serotonin receptors to their normal sensitivity. She used a gut-detoxifying formula, probiotics, and a combination of L-glutamine, gamma-oryzanol, and soothing herbs to help heal her intestine.
Jennifer has been alcohol-free for more than 15 months and experiences absolutely no craving for alcohol. Jennifer describes her own progress as “amazing.”*
Editor’s note: Individuals taking selective serotonin reuptake inhibitor drugs such as Lexapro® should not take 5-HTP.
Susan*
Susan was a 21-year-old woman who came to Dr. Sponaugle’s clinic with her mother. Susan had been drinking two liters of vodka while consuming 1,000 mg of OxyContin® (a narcotic) and 20 mg of Xanax® (an anti-anxiety drug) daily. Susan’s problems had begun at age 12, since which time she had attended eight drug rehab programs at a cost of $240,000.
Susan had begun by raiding her parents’ liquor cabinet to “calm her anxious brain.” Dr. Sponaugle learned that Susan had not experienced anxiety issues prior to age 12, which was also, significantly, the age when she began having her periods, which were always longer and heavier than those of her peers.
Sponaugle recognized in Susan the classic presentation of progesterone deficiency. Her ovaries were producing normal levels of estrogen unopposed by progesterone, a situation known to result in enhanced anxiety.35,36 Her relatively high estrogen levels also boosted dopamine production, further adding to overactivity in Susan’s anxiety-producing brain regions. 37
Like Jennifer, then, Susan began by drinking the most readily-available calming drug she could find: alcohol. Her alcohol consumption contributed to the kind of toxic yeast overgrowth in the gastrointestinal tract that Dr. Sponaugle has found is associated with deficiencies of serotonin and taurine (two calming brain chemicals) in alcoholic patients. Her ensuing leaky gut contributed to elevated brain histamine activity.
Quite naturally, then, Susan turned to stronger drugs that could calm the mounting anxiety levels triggered by excess histamine activity. She discovered the soothing nature of narcotics and the calming influence of the benzodiazepines (such as Xanax®).
Sponaugle began by optimizing Susan’s hormonal levels (the original problem) and balancing her brain chemistry. He aggressively detoxified her gut with natural supplements designed to kill the yeast Candida albicans and other unwanted organisms. And he restored levels of nutrients and minerals that had been deficient.
Susan is now more than three years post-treatment without a single relapse. Says Sponaugle, “She is well on her way to enjoying a wonderful future.”*
Summary

While millions of Americans suffer from chemical addictions, conventional detox, and treatment programs have dismal success, with relapse rates ranging from 50-90%.
Few such wellness programs consider the complicated inherited and acquired abnormalities in brain chemistry associated with addictions, focusing instead on frustrating “talk therapy” or medical detoxification strategies.
Marvin “Rick” Sponaugle, MD, incorporates state-of-the-art brain science and comprehensive biochemical testing to understand each addict’s unique pattern of brain chemistry. He uses this information to determine precisely how and why each person is self-medicating with their drug(s) of choice to achieve what is often the only semblance of “normalcy” they can experience.
With this information and an understanding of integrative health, Sponaugle first detoxifies his patients while administering deficient amino acid brain chemical precursors, vitamins, minerals, and medications to neutralize their uncomfortable adrenaline surges.
He then issues a comprehensive program of biochemical and hormonal balancing to remove the driving forces behind the addiction. Sponaugle’s results speak for themselves: his patients’ relapse rate is just 9%.*
Neurological Conditions
Dr. Sponaugle reports exceptionally successful results with his biochemically-based addiction treatment programs. He has now applied the same principles of detoxification and chemical balancing to other apparently intractable conditions. Among these, the most intriguing is his management of neurological illnesses such as multiple sclerosis (MS), amyotrophic lateral sclerosis (ALS, also called Lou Gehrig’s Disease), attention-deficit/hyperactivity disorder (ADHD), and even Alzheimer’s disease (AD).
Says Sponaugle, “US physicians lag far behind their European counterparts in recognizing the role played by biotoxins, especially those from indoor molds and solvent toxins such as benzene and toluene, in the causation of MS, AD, and other neurological conditions.”
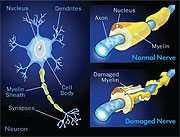
Sponaugle notes that basic science studies have long demonstrated a relationship between mold toxins and MS.38 In MS, brain cells lose their vital insulating sheath of the fat-and-protein material called myelin, leading to the disease's debilitating symptoms.
It is now well documented that fungi, including molds, release toxins, known as mycotoxins that activate immune system cells and trigger them to destroy brain cells.38,39 Nonetheless, says Sponaugle, American physicians continue to tell their patients that the cause of MS is unknown.
There is increasing evidence that fungal toxins are causative in other neurological conditions, including Alzheimer’s disease. In this condition, fungal toxins have been identified in the brain or nerve tissue of sufferers of the disorders.40
Tissue from these patients and those with other neurological disorders also contain high levels of an enzyme that targets the fungal protein called chitin, which is not otherwise found in the human body.41
Molds and their toxins are distressingly prevalent in our food supply. One study demonstrated that nearly 20% of corn samples from the Midwest contained one of the four most dangerous fungal toxins.42
Sponaugle says that one in four Americans, 24%, have a genetic factor that interferes with effectively removing mold and industrial toxins. He sees this genetic factor in 80% of his non-addicted “wellness” patients who suffer common maladies such as chronic fatigue syndrome, fibromyalgia, and even poorly-defined malaise, in addition to neurological conditions such as depression, anxiety, rage, and bipolar symptoms.
Dr. Sponaugle has turned his observations into solid clinical practice. He has designed an aggressive intravenous treatment model for toxin removal that is highly successful at diminishing symptoms of his patients suffering from MS and other debilitating brain disorders such as ALS, Parkinson’s disease, Alzheimer’s disease, and autism.
Non-Addictive Conditions Also Respond
to Sponaugle’s Treatment Approach
Among the many targeted programs Dr. Sponaugle offers, several are aimed at treating non-addictive conditions. These conditions share certain characteristics with addictive disorders, such as producing imbalances in brain chemistry, and often have toxin exposure as a cause. Sponaugle has successfully treated patients with:
- Hypoglycemia
- Food allergies
- Nutrient depletion
- Anxiety/insomnia
- ADD/ADHD (including many high-performing adult professionals)
- Depression
- Multiple sclerosis
- Alzheimer’s disease
- Hormonal imbalance
Sponaugle’s Brain and Body Wellness Program targets those with suspected toxins (especially indoor mold and industrial solvent toxicity) that may be at the root of their disorders.
His comprehensive testing and proprietary intravenous treatment model have successfully managed these conditions.
Addiction Treatment Testimonials
Take a moment to watch these amazing stories of healing and know that we are always ready and eager to make a difference in your life or the life of a loved one who may be battling with addiction.



References:
1. Available at: http://www.whitehousedrugpolicy.gov/publications/pdf/consdrug_fs.pdf. Accessed April 29, 2011.
2. Available at: http://online.wsj.com/article/SB10001424052748704254604574614230731506644.html. Accessed April 29, 2011.
3. Xu J, Kochanek KD, Murphy SL, Tejada-Vera B. Deaths: Final Data for 2007. National Vital Statistics Reports 58/9. Centers for Disease Control and Prevention. National Center for Health Statistics. 2010 May.
4. Available at: http://www.oas.samhsa.gov/spotlight/spotlight021counseling.pdf. Accessed April 29, 2011.
5. Available at: http://www.caron.org/current-statistics.html. Accessed April 28, 2011.
6. Available at: http://www.nida.nih.gov/podat/faqs.html. Accessed April 28, 2011.
7. Sponaugle MR. Brain Chemistry and Addiction. 2011.
8. Office of Applied Studies. Drug Abuse at Highest Level in Nearly a Decade. Rockville, MD: Department of Health and Human Services; December 2010.
9. Available at: http://www.whitehousedrugpolicy.gov/drugfact/prescrptn_drgs/rx_ff.html. Accessed April 28, 2011.
10. Available at: http://www.adolescent-substance-abuse.com/national-drug-statistics.html. Accessed April 28, 2011.
11. Available at: http://www.oas.samhsa.gov/2k10/DAWN034/EDHighlights.htm. Accessed April 28, 2011.
12. Available at: http://oas.samhsa.gov/2k10/DAWN015/IllicitAbuse.cfm. Accessed April 28, 2011.
13. Cosgrove KP. Imaging receptor changes in human drug abusers. Curr Top Behav Neurosci. 2010;3:199-217.
14. Martinez D, Narendran R. Imaging neurotransmitter release by drugs of abuse. Curr Top Behav Neurosci. 2010;3:219-45.
15. Weinstein AM. Computer and video game addiction-a comparison between game users and non-game users. Am J Drug Alcohol Abuse. 2010 Sep;36(5):268-76.
16. Blum K, Chen AL, Chen TJ, et al. Activation instead of blocking mesolimbic dopaminergic reward circuitry is a preferred modality in the long term treatment of reward deficiency syndrome (RDS): a commentary. Theor Biol Med Model. 2008 Nov 12;5:24.
17. George O, Koob GF. Individual differences in prefrontal cortex function and the transition from drug use to drug dependence. Neurosci Biobehav Rev. 2010 Nov;35(2):232-47.
18. Koob GF, Volkow ND. Neurocircuitry of addiction. Neuropsychopharmacology. 2010 Jan;35(1):217-38.
19. Ross S, Peselow E. The neurobiology of addictive disorders. Clin Neuropharmacol. 2009 Sep-Oct;32(5):269-76.
20. Spooren W, Lesage A, Lavreysen H, Gasparini F, Steckler T. Metabotropic glutamate receptors: their therapeutic potential in anxiety. Curr Top Behav Neurosci. 2010;2:391-413.
21. Freitas-Ferrari MC, Hallak JE, Trzesniak C, et al. Neuroimaging in social anxiety disorder: a systematic review of the literature. Prog Neuropsychopharmacol Biol Psychiatry. 2010 May 30;34(4):565-80.
22. Koh KB, Kang JI, Lee JD, Lee YJ. Shared neural activity in panic disorder and undifferentiated somatoform disorder compared with healthy controls. J Clin Psychiatry. 2010 Dec;71(12):1576-81.
23. Nikolaus S, Antke C, Beu M, Muller HW. Cortical GABA, striatal dopamine and midbrain serotonin as the key players in compulsive and anxiety disorders—results from in vivo imaging studies. Rev Neurosci. 2010;21(2):119-39.
24. Bonini JS, Da Silva WC, Da Silveira CK, Kohler CA, Izquierdo I, Cammarota M. Histamine facilitates consolidation of fear extinction. Int J Neuropsychopharmacol. 2011 Jan 7:1-9.
25. Dere E, Zlomuzica A, De Souza Silva MA, Ruocco LA, Sadile AG, Huston JP. Neuronal histamine and the interplay of memory, reinforcement and emotions. Behav Brain Res. 2010 Dec 31;215(2):209-20.
26. Zarrindast MR, Nasehi M, Khansari M, Bananej M. Influence of nitric oxide agents in the rat amygdala on anxiogenic-like effect induced by histamine. Neurosci Lett. 2011 Feb 1;489(1):38-42.
27. Katsui R, Kuniyasu H, Matsuyoshi H, Fujii H, Nakajima Y, Takaki M. The plasticity of the defecation reflex pathway in the enteric nervous system of guinea pigs. J Smooth Muscle Res. 2009 Feb;45(1):1-13.
28. Maes M. The cytokine hypothesis of depression: inflammation, oxidative & nitrosative stress (IO&NS) and leaky gut as new targets for adjunctive treatments in depression. Neuro Endocrinol Lett. 2008 Jun;29(3):287-91.
29. Maes M, Yirmyia R, Noraberg J, et al. The inflammatory & neurodegenerative (I&ND) hypothesis of depression: leads for future research and new drug developments in depression. Metab Brain Dis. 2009 Mar;24(1):27-53.
30. Mendoza C, Matheus N, Iceta R, Mesonero JE, Alcalde AI. Lipopolysaccharide induces alteration of serotonin transporter in human intestinal epithelial cells. Innate Immun. 2009 Aug;15(4):243-50.
31. Durant C, Christmas D, Nutt D. The pharmacology of anxiety. Curr Top Behav Neurosci. 2010;2:303-30.
32. Goodman A. Neurobiology of addiction. An integrative review. Biochem Pharmacol. 2008 Jan 1;75(1):266-322.
33. Schule C, Eser D, Baghai TC, Nothdurfter C, Kessler JS, Rupprecht R. Neuroactive steroids in affective disorders: target for novel antidepressant or anxiolytic drugs? Neuroscience. 2011 Mar 23.
34. Kugaya A, Epperson CN, Zoghbi S, et al. Increase in prefrontal cortex serotonin 2A receptors following estrogen treatment in postmenopausal women. Am J Psychiatry. 2003 Aug;160(8):1522-4.
35. Frye CA, Sumida K, Dudek BC, et al. Progesterone’s effects to reduce anxiety behavior of aged mice do not require actions via intracellular progestin receptors. Psychopharmacology (Berl). 2006 Jun;186(3):312-22.
36. Reddy DS, O’Malley BW, Rogawski MA. Anxiolytic activity of progesterone in progesterone receptor knockout mice. Neuropharmacology. 2005 Jan;48(1):14-24.
37. Morissette M, Levesque D, Di Paolo T. Effect of chronic estradiol treatment on brain dopamine receptor reappearance after irreversible blockade: an autoradiographic study. Mol Pharmacol. 1992 Sep;42(3):480-8.
38. Purzycki CB, Shain DH. Fungal toxins and multiple sclerosis: a compelling connection. Brain Res Bull. 2010 Apr 29;82(1-2):4-6.
39. Hiestand PC, Rausch M, Meier DP, Foster CA. Ascomycete derivative to MS therapeutic: S1P receptor modulator FTY720. Prog Drug Res. 2008;66:361, 363-81.
40. Sotgiu S, Musumeci S, Marconi S, Gini B, Bonetti B. Different content of chitin-like polysaccharides in multiple sclerosis and Alzheimer’s disease brains. J Neuroimmunol. 2008 Jun 15;197(1):70-3.
41. Barone R, Sotgiu S, Musumeci S. Plasma chitotriosidase in health and pathology. Clin Lab. 2007;53(5-6):321-33.
42. Russell L, Cox DF, Larsen G, Bodwell K, Nelson CE. Incidence of molds and mycotoxins in commercial animal feed mills in seven midwestern states, 1988-1989. J Anim Sci. 1991 Jan;69(1):5-12.